
 Welcome to June 2026! June brings the official start of summer for the Northern Hemisphere, longer days, the summer solstice and Father’s Day. As the saying goes, “The best time to plant a tree was 20 years ago. The second best time is now.” While a lot of the year is behind us, now is the perfect time to carpe diem. While we have made tremendous progress so far, I need your continued partnership to make the most of the opportunities we have in front of us for the rest of 2026.
Welcome to June 2026! June brings the official start of summer for the Northern Hemisphere, longer days, the summer solstice and Father’s Day. As the saying goes, “The best time to plant a tree was 20 years ago. The second best time is now.” While a lot of the year is behind us, now is the perfect time to carpe diem. While we have made tremendous progress so far, I need your continued partnership to make the most of the opportunities we have in front of us for the rest of 2026.
- Stroke Response Reminder: Timely Escalation and Responsibilities. We have experienced a number of safety events involving patients who developed stroke symptoms with delayed or incomplete escalation. Please take a look at the document at the bottom for some reminders about Code Stroke. An important note: Code Stroke DOES NOT automatically initiate a Tele-Stroke or Neurology Consult – the attending physician/APC is responsible for initiating the consult and can use HUCs as needed to page those teams.
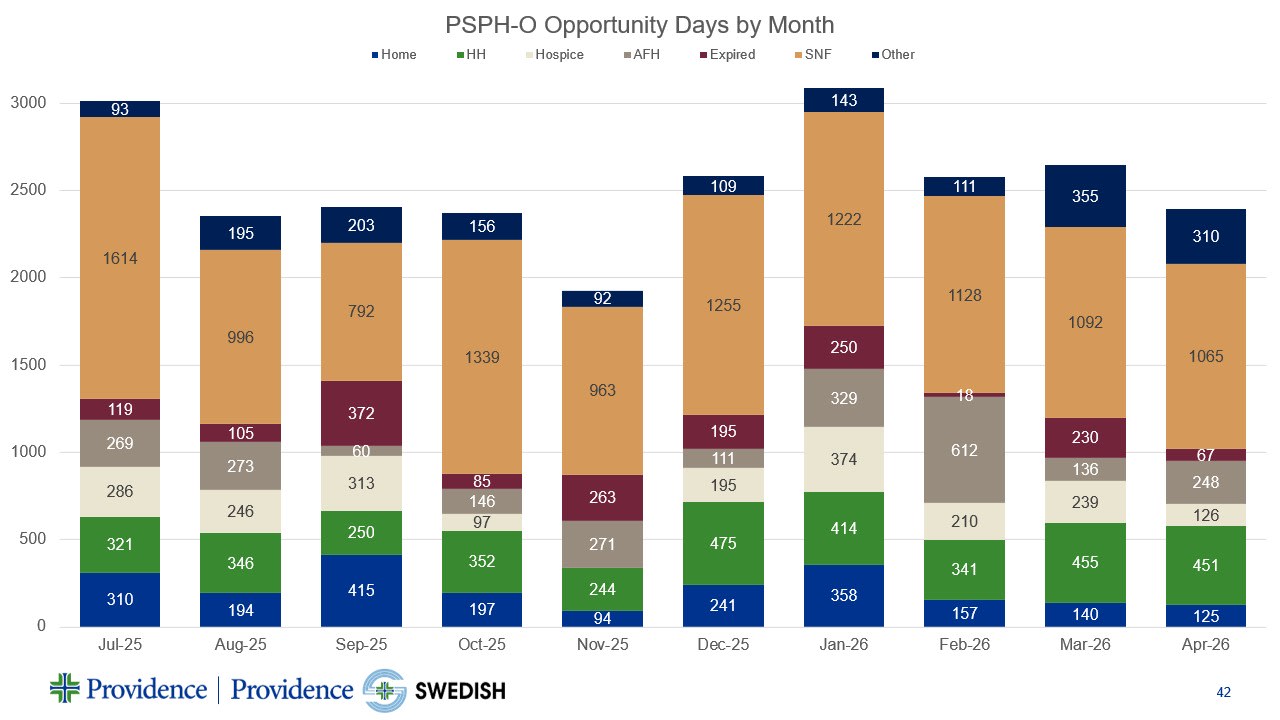
- Length of Stay and Opportunity Days (ODs): We have made tremendous progress, but opportunity remains around patients discharging to Home and to Skilled Nursing Facility (SNF). An “opportunity day (OD)” is an extra day of stay past the Geometric Mean Length of Stay (GMLOS) and/or stay beyond medically ready. See the graphic below for some takeaways around our “opportunity days.”
-
-
Look at our progress around opportunity days to home… strong work, but more to go! Remember 2/3 to 3/4 of our patients go home. Save ODs here by talking about home and planning for home from admission. Home is a preferred location for many of our patients… ask “Why not home, why not today” for medically ready patients.
-
Our biggest bucket of ODs remains patients discharging to SNF, especially at PSPH. We discharge more patients to SNF than other comparable sized facilities and get more denials than any other service area. For patients who need SNF, partner early to be sure they meet criteria and timing is closely coordinated with our Care Management team around authorization and documentation. Here each extra day matters!
-
Stroke Response Reminder: Timely Escalation and Physician and APC Responsibilities
We have recently experienced several safety events across both the inpatient setting and ED involving patients who developed stroke symptoms with delayed or incomplete escalation. This serves as an important reminder of our shared expectations for rapid recognition and response to potential stroke.
At our organization, any new BEFAST symptoms or an increase in NIHSS by ≥4 points should be treated as an emergent change. Nursing teams are expected to activate a Code Stroke when these criteria are met.
A few key points:
- Code Stroke activation triggers system workflows (response team notification and CT readiness), but it does not automatically initiate a telestroke or neurology consult.
- If indicated, the attending physician/APC is responsible for initiating the consult (telestroke or neurology.) We can utilize HUCs to help page those teams.
- During high-volume or competing demands, you may initiate telestroke prior to arriving at bedside to avoid delays.
- If you determine that a Code Stroke should not proceed, it remains essential that a timely bedside assessment is completed by the attending. Please also document indication for canceled code stroke.
To support consistency and confidence in recognition, updated nursing tools for stroke assessment and activation are being rolled out this week, aimed at improving specificity and standardization of Code Stroke initiations.
Timely evaluation, clear communication, and adherence to workflows are critical to ensuring optimal patient outcomes.
If you have questions or would like further clarification on stroke protocols, please reach out to:
- Dr. Madeline Nguyen, Medical Director (PSPH)
- Lara Lieberman, RN, Sr. Manager, Stroke Programs (PSPH & PCH)
Thank you for your continued commitment to patient safety and high-quality stroke care.













